

Crossing the Continuum: Providing Outpatient Care in a Bone Marrow Transplant Clinic
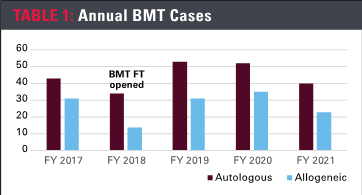
Now more than ever, improving patient outcomes, workflow efficiencies, patient/staff satisfaction and profitability are top priorities in the ever-changing landscape of health care. As reimbursements are tied to many of these metrics, institutions have been charged with developing innovative models of care that travel from the inpatient to the outpatient setting. The Bone Marrow Transplant Fast Track (BMT FT) Clinic is one such program. The clinic opened in August 2018, logging approximately 1,000 patient visits annually since it began operations. An interprofessional team grounded in strong nurse-physician collaboration set the foundation for the program. A 32-bed inpatient hematology/bone marrow transplant unit converted two inpatient rooms to four outpatient chairs to better serve patients post-stem cell transplant (SCT). After patients receive their hematopoietic transplant, they undergo a traditional discharge from their inpatient stay. Oftentimes patients that require the most intense follow-up, which is approximately five to seven visits per week, will be assigned subsequent outpatient appointments in the BMT FT Clinic. The continuity of care allows the patient and care team to follow post-transplant patients closely, identifying clinical issues early and providing swift interventions. With a focus on continuity of care, nurses that take care of patients undergoing transplants on the inpatient side of this unit are also assigned to these patients in the clinic’s ambulatory portion. This model sought to increase patient satisfaction and compliance with post-transplant follow-up, reduce readmissions and length of stay, and identify any post-transplant complications as early as possible.
Patient flow
The BMT FT Clinic was created as a next step after the inpatient setting where daily transfusion/electrolyte administrations were a necessity, but an overnight admission could be phased out if daily needs could be accommodated elsewhere. The outpatient cancer clinic could not guarantee infusion chairs for full days or every day, and often “fresh” (immediate post-discharge) allogeneic BMT patients can require anywhere from four to 10 hours of infusion needs or even a re-admission if hemodynamically unstable. By creating the clinic, four patients were able to be seen every morning with the capability of seeing up to eight patients per day. An algorithm was created to admit a patient to inpatient status if a lab result, symptom or vital sign is flagged as too critical. The BMT FT RN is in close communication with the advance practice provider (APP), charge RN and hospital patient placement to facilitate a quick admission to an open inpatient room, maintaining patient safety. In the converse, if the unit census is high and emergent needs for inpatient beds for patients were indicated, a BMT FT unit would be converted back into two inpatient beds as determined by an algorithm created to suggest this change.
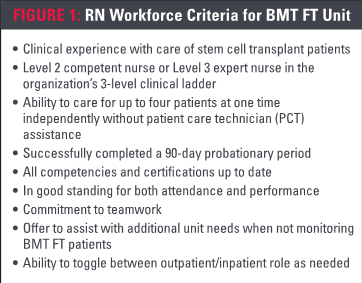
An interprofessional care team was assembled to develop workflows for stem cell transplant patients. However, first the team defined the criteria that would guide the competencies and skills necessary for RNs who could work in both the BMT FT and the inpatient setting. The RN criteria included (Figure 1) clinical experience with care of SCT patients, the ability to care for up to four patients at one time independently without patient care technician assistance and a commitment to teamwork. The BMT FT team is staffed with attending physicians, APPs, a pharmacist, designated staff RNs, an inpatient RN unit director, an assistant RN unit director and an oncology clinical nurse specialist, in addition to hospital support services.
Logistics
Logistics that guide operations and safe clinical practice include strict room cleaning protocols before and after patient visits, as well as daily supply replenishment, quarterly re-education/updates via meetings including BMT FT RNs, APPs, and unit leadership. A BMT FT resource binder lists important phone numbers, use of ambulatory EMR flowsheets, laboratory protocol, as well as how to release BMT FT order sets. Utilization of nurse-driven protocols and the ability to schedule upcoming appointments for staffing purposes were important efforts to standardize care during and after the BMT encounter. Supplies include four infusion chairs and supplies needed to use them. The communication plan includes the use of consistent smart phones assigned to RNs, secure messages to inpatient BMT APPs and ongoing coordination with the unit charge RN for changes in patient status and acuity, in order to anticipate patient/staffing needs.
Workflow
On the day of discharge, the SCT patient and caregiver are given a long-term visitor pass allowing them to bypass security for three months and directly enter the clinic. Utilizing this pass, the patient and one consistent caregiver will arrive and check in with the unit clerk, who will notify the designated BMT FT RN that the patient has arrived. The RN prints out the patient’s ID band, assigns them to a room/chair, assesses vital signs and performs a physical assessment. An IV tube is inserted, blood is drawn for tests and sent “STAT” to the inpatient laboratory, followed by administration of IV fluids, blood products, electrolyte infusions and other prescribed treatments. The physician/APP will visit the patient, begin interventions such as symptom management, as well as communicate a discharge plan, follow-up and next appointment. The patient receives an after-visit summary with instructions at the end of the appointment.
Specialized training
Training for this clinical model includes shadowing an experienced BMT FT RN for several shifts. The inpatient assignments for BMT FT RNs are adjusted accordingly. If an RN has two scheduled BMT FT patients, then that RN is assigned one inpatient; if an RN has one scheduled BMT FT patient, then that RN is assigned two inpatients. BMT FT RNs have to learn ambulatory charting using a different EMR, flowsheets and insurance concerns. Discharged inpatients are scheduled in the BMT FT clinic for multiple appointments in the upcoming weeks for close follow-up. The BMT FT clinic is open from 7 a.m. to 4 p.m. with appointment times offered within that time frame. RN-driven replacement protocols were developed to initiate treatment such as potassium and magnesium supplementation and packed red blood cell and platelet transfusions. Ambulatory infusion guidelines and practices such as faster potassium and magnesium IV infusion were adopted. The Joint Commission and The Foundation for the Accreditation of Cellular Therapy guidelines have been utilized as the standard for safe and expert care in the BMT FT. As this model has shown its value, emergent therapies such as CAR-T cell therapies, mobilization chemotherapy and colony-stimulating factor administration have been used. Inpatient unit staffing was adjusted and communicated with the clinical staffing office to accommodate higher census due to volume and acuity of the fluctuating BMT FT census. Institutional review board-exempt status was acknowledged and approved to share data/results at professional nursing conferences.
Results
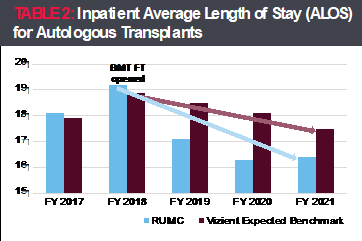
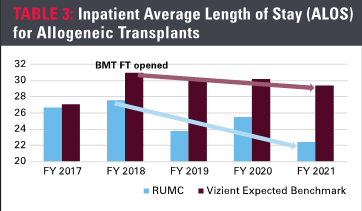
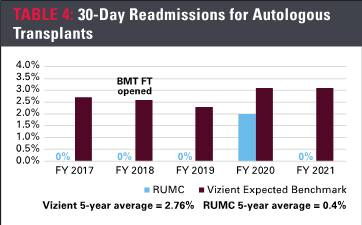
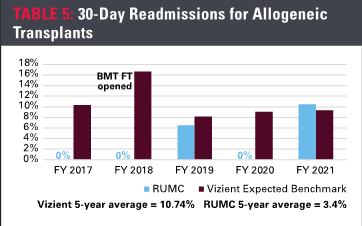
Several key outcomes are measured to define success. Internal baseline data collected in fiscal year 2017 (FY 17) were used as a comparison for the following years. Additionally, Vizient national benchmarking data measuring the same parameters also were used to compare to our internal data over a four-year period (FY 18-FY 21). Table 2 highlights the trends noted from FY 18-FY 21 showing a statistically significant reduction in the average length of stay (ALOS) for patients undergoing autologous transplantation. Similarly, Table 3 showcases a statistically significant reduction in the ALOS for patients undergoing allogeneic transplantation, who often have a much more complicated pathway to successful discharge from the inpatient hospital stay and full recovery. Table 4 depicts a statistically significant decrease in the 30-day readmission rate for patients undergoing autologous transplantation. Finally, Table 5 summarizes a statistically significant reduction in the 30-day readmission rate for patients undergoing allogeneic transplantation. All of these results led to significant cost savings over those years for the organization. Our results also led to an increase in our overall market share, reinforcing our reputation as a regional and national center for excellence.
The clinic has generated positive outcomes for patients and staff. Positive impacts for our nurses included increased job satisfaction in seeing former inpatients successfully transition to ambulatory care, observing them recover and returning to their former selves. Nurses also benefited from improved workflows and efficiency. With a second RN assigned to manage the time-constrained workload, nurses have opportunities for variation from inpatient care and to learn information related to BMT-specific patient population. They reported a renewed sense of excitement with ambulatory practices, interventions and treatments. Positive impacts for our BMT FT patients included the metrics previously discussed, as well as sooner-than-expected inpatient discharge, continued relationships after discharge with their inpatient nurses, expert support and care in an ambulatory environment and continuity of care. They also benefited from returning home, sleeping in their own beds, eating their preferred food and being surrounded with loved ones.
Opportunities for improvement
While the model shows promise, it also presented some downsides for nurses who worked in both outpatient and inpatients areas of the clinic. For instance, some nurses found it hard to transition back to the higher-stress impatient care in the middle of a 12-hour shift and sometimes they did not have sufficient time to emotionally process the BMT FT experience before moving to an inpatient assignment. Some also found it difficult to move to a full inpatient assignment after BMT FT visits were completed. Unit leaders are considering improving operations by assigning just one nurse to FT operations daily with no inpatient/outpatient combination assignments. However, because the clinic’s volumes are limited by space, to do so now would not be an efficient use of staff.
Downsides for BMT FT patients include dependence on a support person for transportation and other needs, the support person having to wait while their loved one is receiving treatment, limited control over appointment dates/times and costs accrued. The frequency of appointments, often daily or every other day, also can be a hardship. The clinic offers patients great flexibility in their appointment times to increase their satisfaction based on individual factors, such as traffic considerations and distance to travel in an effort to mitigate these difficulties.
At the organizational level, leaders are pointing out the need to dedicate a clinic budget that is separate from the inpatient setting – both from a revenue and expense perspective. The clinic’s quality and financial successes have helped leaders advocate for resources needed to promote replication and growth, in an effort to improve service to this population. Information on patient volume and the productive nursing hours utilized to care for this patient population has been collected manually and leaders are working towards incorporating the financial elements in the FY 23 operational budget.
Looking ahead
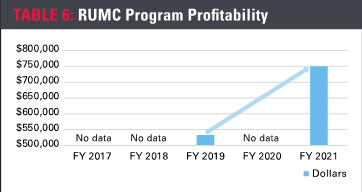
While not all interventions have been fully measured, we know the impact of this BMT FT clinic has been impressive. Recent data suggest that the ALOS for both autologous and allogeneic transplants has been reduced, readmissions have been reduced in the allogeneic transplant population and program profitability has increased (Table 6). A slight increase was seen in the readmission rate for the autologous transplant population compared to our previous years’ data, but still a significant reduction when compared to the national data. It has been a huge satisfier for the patients, caregivers, nurses and providers delivering their care. This program has created an easy transition for patients and their caregiver(s), contributing positively to their patient experience. In addition to the positive impact on patient care, this project provided nursing at all levels the opportunity to support and collaborate on an innovative care team model.
Acknowledgments
The authors would like to thank the following individuals for their assistance with this manuscript: Erin Dowding, MSN, APRN, ACNS-BC, clinical nurse specialist, inpatient oncology; Hayley Lesnik, BSN, RN, BMTCN, co-lead Bone Marrow Transplant Fast Track Clinic; and Jamie Schanz, BSN, RN, OCN, co-lead Bone Marrow Transplant Fast Track Clinic, at Rush University Medical Center, Chicago.
ABOUT THE AUTHORS
Diane Jakubik, MA, RN, CMSRN, is unit director, stem cell transplant/hematology.
Eric Zack, DNP, RN, BMTCN, is a staff nurse.
Katherine Quinlan, BSN, RN, BMTCN, is assistant unit director, stem cell transplant/hematology.
Aney Abraham, DNP, RN, NE-BC, is vice president of patient care services.
All work at Rush University Medical Center, Chicago.